Precise staging without radical lymphadenectomy — using NIR/ICG fluorescence technology.
Endometrial cancer develops in the uterine cavity, specifically in the endometrium (inner lining). Its incidence in North America and Western Europe is 9.9–15 new cases per 100,000 women annually.
It typically occurs in postmenopausal women and often presents with early symptoms (vaginal bleeding), resulting in diagnosis at an early stage in most cases.
The primary treatment is total hysterectomy with bilateral salpingo-oophorectomy. Depending on the stage, radiotherapy and/or chemotherapy may be recommended. Overall survival in stage I is high, with more than 80% of women disease-free five years after surgery.
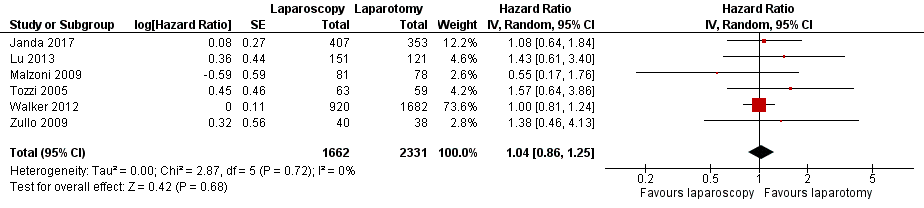
Nine large randomized trials have demonstrated that laparoscopy is associated with reduced surgical morbidity and equivalent oncological outcomes (overall survival and disease-free survival). Specifically, it is associated with less blood loss and shorter hospital stay.
Lymph node metastases are found in one out of ten women who appear to have cancer confined to the uterus. Systematic lymphadenectomy provides prognostic information but has not been shown to improve survival, while being associated with serious complications such as lymphedema. The ideal solution is to obtain this information without the downsides of radical removal.
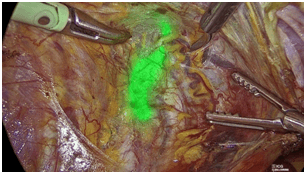
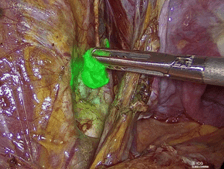
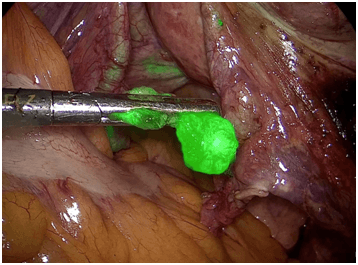
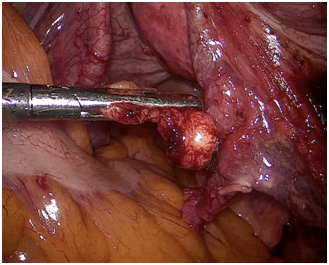
Indocyanine green (ICG) is a fluorescent dye approved by the FDA (2018) for lymphatic vessel imaging in endometrial and cervical cancer. After injection into the cervix, it travels through lymphatic vessels to the pelvic lymph nodes, which fluoresce under NIR illumination. The surgeon identifies and removes them without radical lymphadenectomy.
The largest multicenter prospective study (FIRES, Rossi et al., Lancet Oncology, 2017) involving 344 patients showed a sensitivity of 97.2% with a false-negative probability of 2.8%.
The technique has been applied at the Center for Gynecological Surgery (MITERA Crete) since February 2023 using the RUBINA 4K-3D system.